United Therapeutics Announces Additional Results From FREEDOM-EV Study Showing The Hemodynamic And Risk Status Reduction Benefits Of Orenitram Treatment In Patients With Pulmonary Arterial Hypertension
- Orenitram demonstrated improvement in hemodynamic parameters and risk status, important indicators of long-term outcomes in PAH patients, in presentations at recent scientific conferences
- Separately, total PAH-related patient healthcare costs are 67% higher for selexipag in article published in Drugs - Real World Outcomes
Orenitram was originally approved by the
The recent publications add further to the evidence showing the benefits of treatments with Orenitram in PAH patients:
- Data from the FREEDOM-EV hemodynamic sub-study showing that Orenitram significantly improved key hemodynamic parameters, including pulmonary vascular resistance (20% reduction), cardiac output (19% increase), and cardiac index (17% increase), at a median week 24 dose of 5.5 mg three times daily were recently presented at the
Pulmonary Vascular Research Institute (PVRI) 14th AnnualWorld Congress on Peripheral Vascular Disease (PVD).1 - Analyses of the FREEDOM-EV study showing that Orenitram significantly improved patient risk status assessed by two different methodologies (REVEAL 2.0 and French noninvasive), which can be predictor of clinical worsening and survival, were accepted for presentation at the
American Thoracic Society (ATS) 2020International Conference .2,3 - A retrospective database analysis of
U.S. health insurance claims concluding that treatment with selexipag was associated with 67% higher PAH-related patient healthcare costs compared to Orenitram despite similar adherence, persistence, and rate of PAH-related hospitalizations was recently published in the journal Drugs – Real World Outcomes.4,5,6 (Comparison of products does not imply clinical comparisons of safety or efficacy.)
"FREEDOM-EV demonstrated that Orenitram treatment not only delays disease progression, but also leads to durable improvement in clinically relevant components of risk, including six-minute walk distance, NT-proBNP, and functional class," said
"Data from the FREEDOM-EV study have resonated well with PAH providers and payers," said
Newly published data are summarized below. Please refer to the respective publications for further information.
Significant Impact on Hemodynamics – Data from the FREEDOM-EV Study
FREEDOM-EV was a phase III, international, multi-center, randomized, double-blind, placebo- controlled, event-driven study of Orenitram in patients with PAH receiving background oral monotherapy (N=690).7,8 Orenitram decreased the risk of adjudicated clinical worsening events by 25% compared to placebo (hazard ratio: 0.75; p=0.039). These results were largely driven by a 61% decrease in the risk of disease progression compared to placebo (hazard ratio: 0.39; p=0.0002).
The hemodynamic sub-study included 61 patients who volunteered for right heart catheterization at baseline and study Week 24.1,9 Patients were predominantly female (75%) and received background phosphodiesterase type 5 inhibitor, soluble guanylate cyclase stimulator (85%), or endothelin receptor antagonist (15%) therapy.
At Week 24, the median (interquartile range) Orenitram dose achieved was 5.5 (3.5, 6) mg three times daily (TID). Treatment with Orenitram resulted in significant changes in hemodynamic parameters at Week 24, including a:
- 20% reduction in pulmonary vascular resistance (PVR; p=0.0241);
- 21% reduction in pulmonary vascular resistance index (PVRI; p=0.0295);
- 19% increase in cardiac output (CO; p=0.0051);
- 17% increase in cardiac index (CI; p=0.0128); and
- 13% increase in stroke volume (SV; p=0.043).
There were no significant changes in other hemodynamic parameters, including mean right atrial pressure (RAPm), pulmonary artery wedge pressure (PAWPm), pulmonary artery pressure (PAPm), or heart rate (HR) between the Orenitram and placebo groups. Data set are represented in the table below.
The most common adverse reactions reported were consistent with the parent study and included headache, diarrhea, flushing, nausea, and vomiting.
Data are limited by the relatively small sample size compared to the parent study (61 patients v. 690 patients). Authors note that baseline patient characteristics were similar; however, median Orenitram dose achieved was higher in hemodynamic sub-study patients (5.5 mg TID vs. 3.56 mg TID, overall).

Significant Impact on Risk – Data from the FREEDOM-EV Study
Orenitram demonstrated a robust impact on key measures of disease status in the FREEDOM-EV study, including functional class, NT-proBNP levels, and French noninvasive risk profile.7,8 Those treated with Orenitram exhibited a statistically significant improvement in French noninvasive risk profile compared to placebo through study Week 60. This is of particular note, as despite seemingly balanced characteristics, placebo-assigned participants were found to be at lower risk at baseline (p=0.002).
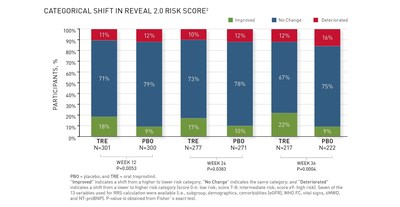
Thus, a post-hoc analysis of FREEDOM-EV was performed to determine the impact of Orenitram on the REVEAL 2.0 risk score (RRS).2 At baseline, 53%, 26%, and 21% of Orenitram subjects were in low (score 0-6), intermediate (score 7-8), and high-risk (score ≥9) categories, respectively, compared with 61%, 21%, and 18% of placebo subjects, respectively. The baseline RRS distribution was not statistically different between groups (p=0.0831), although mean scores between the groups were (6.3 Orenitram vs. 5.83 placebo; p=0.0107). Compared to baseline, there was a statistically significant improvement in RRS category in those treated with Orenitram compared to placebo through Week 36 (see figure, beyond Week 36 not presented). At Week 36, the mean RRS in participants treated with Orenitram decreased by 0.61, compared to a decrease of 0.01 in participants treated with placebo (mean difference: -0.599; p=0.002).
To further assess the impact of the imbalance in patient risk in FREEDOM-EV, primary endpoint results were alternatively adjusted by baseline risk score.3 That is, the primary endpoint was corrected for the imbalance in baseline patient risk. Adjusting the primary endpoint analyses by baseline risk score magnified the treatment effect already observed in the pre-specified analysis (a 25% reduction in clinical worsening with Orenitram; hazard ratio: 0.75; p=0.039). Adjusting by the French noninvasive methodology, Orenitram was found to decrease the risk of clinical worsening events by 39% compared to placebo (hazard ratio: 0.61; p=0.0006). Adjusting by RRS (as a continuous variable), Orenitram decreased the risk of clinical worsening events by 33% compared to placed (hazard ratio: 0.67; p=0.0047).
The authors comment that risk scores appear to be a robust stratification tool and may be more sensitive for detecting treatment effects than traditional stratification factors.
Assessment of patient risk status via French noninvasive methodology was prespecified as an exploratory analysis in the FREEDOM-EV statistical analysis plan. Additional evaluations on patient risk were conducted post-hoc and should be regarded with appropriate caution.
Cost Effectiveness – Data from a
A total of 256 patients with PAH receiving oral prostacyclin therapy were included in this retrospective database analysis (130 Orenitram and 126 selexipag patients).4,5,6 Various outcomes were evaluated over a six-month follow-up period, including adherence to treatment, persistence on treatment, all-cause and PAH-related hospitalizations, as well as healthcare costs.
Adherence, persistence, and hospitalization outcomes were comparable between patient groups. Treatment adherence was measured using the medication possession ratio (MPR) and the proportion of days covered (PDC). Mean MPR was higher for Orenitram patients (p=0.039), but there were no significant differences in the proportion of patients with ≥80% mean MPR, mean PDC, or ≥80% PDC between groups. Also, there was no significant difference between groups in the proportion of patients persistent on treatment, when discontinuation was defined as a gap in treatment of either ≥30 or ≥60 days. Mean number of all-cause outpatient visits was higher with Orenitram (p<0.001). However, there was no significant difference between groups in number of all-cause and PAH-related hospitalizations, length of hospital stay, or number of emergency department visits.
Healthcare costs differed significantly between the treatment groups. Treatment with selexipag was associated with 51.4% higher mean total healthcare costs compared to Orenitram (mean difference of
The authors acknowledge the relatively small sample size included in the analysis and various health insurance claims database limitations, including inability to ascertain patient PAH disease severity, whether patients take medication as prescribed, and medication dose changes.
About FREEDOM-EV
FREEDOM-EV was a phase III, international, multi-center, randomized, double-blind, placebo- controlled, event-driven clinical worsening study of oral treprostinil in patients with PAH receiving background oral monotherapy (a phosphodiesterase type 5 inhibitor, an endothelin receptor antagonist, or a soluble guanylate cyclase stimulator).7 The primary endpoint of this study was met, as Orenitram decreased the risk of adjudicated clinical worsening events by 25% compared to placebo (p=0.039). These results were largely driven by delay in disease progression; Orenitram decreased the risk of disease progression by 61% compared with placebo (p=0.0002).
Global enrollment was completed in
Secondary Endpoints
Secondary endpoints included changes from baseline in 6MWD, Borg dyspnea score (shortness of breath test), functional class, NT-proBNP levels, and combined 6MWD and Borg dyspnea score. Secondary endpoint data, which are not included in the FDA-approved labeling, are summarized below:
- Change in 6MWD: The median 6MWD trended toward improvement at week 24 (Hodges-Lehmann treatment estimate: 7 meters). Median 6MWD improved with Orenitram at weeks 36 (13 meters) and 48 (21 meters) compared to placebo. Six-minute walk distance at week 24 was not significantly different from placebo.
- Change in Borg dyspnea score and
World Health Organization (WHO) functional class: When classified categorically as 'improved', 'no change', or 'deteriorated', participants in the Orenitram group exhibited a significantly positive shift in Borg dyspnea score and WHO functional class compared to placebo at weeks 24, 36, and 48. - Change in NT-proBNP levels: NT-proBNP levels were significantly improved with Orenitram at weeks 24 and 36. Per protocol, NT-proBNP was not assessed at week 48.
- Change in combined 6MWD and Borg dyspnea score: Combined 6MWD and Borg dyspnea score was significantly improved with Orenitram when assessed at week 24 compared to placebo.
Vital Status Sub-study
In FREEDOM-EV, vital status was collected throughout the study from patients who agreed to be followed. This included patients who discontinued early and those who transitioned to the open-label continuation study. When vital status was collected, cause of death was not specified.
Mortality was similar between Orenitram and placebo groups at the end of randomized treatment and the open label extension. However, in participants for which data are available (89%; unknown for 43 Orenitram and 31 placebo patients), Orenitram was associated with a 37% decreased risk of mortality compared with placebo at study closure. This mortality data is not reflected in the FDA-approved label, since it includes data accrued in the open-label extension study. Due to data collection limitations, data must be interpreted cautiously.
References
1. White RJ, Bohns Meyer GM, Pulido T, et al. Treatment with oral treprostinil improves hemodynamics in participants with PAH. Presented at: PVRI 14th Annual
2. Benza RL, Gomberg-Maitland M, Farber HW, et al. An analysis of FREEDOM-EV using the French noninvasive and REVEAL 2.0 risk stratification criteria. Accepted to:
3. Benza RL, Gomberg-Maitland M, Farber HW, et al. The impact of stratification by baseline pulmonary arterial hypertension risk score – analysis from the FREEDOM-EV study. Accepted to:
4. Dean BB, Saundankar V, Stafkey-Mailey D, et al. Medication Adherence and Healthcare Costs Among Patients with Pulmonary Arterial Hypertension Treated with Oral Prostacyclins: A Retrospective Cohort Study. Drugs – Real World Outcomes. 2020
5. Dean BB. Healthcare costs lower with treprostinil versus selexipag for PAH.
6. Wexler M. Orenitram tablets more cost-effective than Uptravi as PAH treatment, study suggests.
7. White RJ,
8. Bryson S. Orenitram slows PAH progression when used with other therapies, Phase 3 trial finds.
9. Data on file.
About Orenitram
Indication
Orenitram is a prostacyclin mimetic indicated for treatment of pulmonary arterial hypertension (PAH;
Important Safety Information for Orenitram
CONTRAINDICATIONS
- Avoid use of Orenitram in patients with severe hepatic impairment (Child
Pugh Class C ) due to increases in systemic exposure.
WARNINGS AND PRECAUTIONS
- Abrupt discontinuation or sudden large reductions in dosage of Orenitram may result in worsening of PAH symptoms.
- The Orenitram tablet shell does not dissolve. In patients with diverticulosis, Orenitram tablets can lodge in a diverticulum.
ADVERSE REACTIONS
- In the 12-week, placebo-controlled, monotherapy study, and an event-driven, placebo- controlled, combination therapy study, adverse reactions that occurred at rates at least 5% higher on Orenitram than on placebo included headache, diarrhea, nausea, vomiting, flushing, pain in jaw, pain in extremity, hypokalemia, abdominal discomfort, and upper abdominal pain.
DRUG INTERACTIONS
- Co-administration of Orenitram and the CYP2C8 enzyme inhibitor gemfibrozil increases exposure to treprostinil; therefore, Orenitram dosage reduction may be necessary in these patients.
SPECIFIC POPULATIONS
- Animal reproductive studies with Orenitram have shown an adverse effect on the fetus. There are no adequate and well-controlled studies with Orenitram in pregnant women.
- It is not known whether treprostinil is excreted in human milk or if it affects the breastfed infant or milk production.
- Safety and effectiveness of Orenitram in pediatric patients have not been established.
- Use of Orenitram in patients aged 65 years and over demonstrated slightly higher absolute and relative adverse event rates compared to younger patients. Caution should be used when selecting a dose for geriatric patients.
- There is a marked increase in the systemic exposure to treprostinil in hepatically impaired patients.
Please see Full Prescribing Information and Patient Information at www.orenitram.com or call 1-877-UNITHER (1-877-864-8437).
About
Through our wholly-owned subsidiary, Lung Biotechnology PBC, we are focused on addressing the acute national shortage of transplantable lungs and other organs with a variety of technologies that either delay the need for such organs or expand the supply. Lung Biotechnology is the first public benefit corporation subsidiary of a public biotechnology or pharmaceutical company.
Forward-looking Statements
Statements included in this press release that are not historical in nature are "forward-looking statements" within the meaning of the Private Securities Litigation Reform Act of 1995. Forward-looking statements include, among others, statements regarding the impact of the FREEDOM-EV results on physicians, payers and patients, and the commercial potential for Orenitram. These forward-looking statements are subject to certain risks and uncertainties, such as those described in our periodic and other reports filed with the
ORENITRAM is a registered trademark of
Investor contact:
[email protected]
(202) 919-4097
Media contacts:
[email protected] / [email protected]
(212) 300-8315 / (212) 300-8364
![]() View original content to download multimedia:http://www.prnewswire.com/news-releases/united-therapeutics-announces-additional-results-from-freedom-ev-study-showing-the-hemodynamic-and-risk-status-reduction-benefits-of-orenitram-treatment-in-patients-with-pulmonary-arterial-hypertension-301045819.html
View original content to download multimedia:http://www.prnewswire.com/news-releases/united-therapeutics-announces-additional-results-from-freedom-ev-study-showing-the-hemodynamic-and-risk-status-reduction-benefits-of-orenitram-treatment-in-patients-with-pulmonary-arterial-hypertension-301045819.html
SOURCE
Recent Press Releases
29 Jul 2026
United Therapeutics Corporation Announces ADVANCE OUTCOMES Study of Ralinepag Published in The Lancet23 Jul 2026
United Therapeutics Corporation Announces Appointment of Victor Dzau to its Board of Directors27 May 2026
United Therapeutics Corporation to Present at the Jefferies Global Healthcare Conference